Phase 1: Intervention development and co-production
Phase 1 focused on understanding why people put off attending routine dental care and using these insights to help develop an intervention that could be delivered during urgent dental care appointments. This phase combined theory synthesis, in-depth qualitative research and extensive patient and public involvement to ensure that RETURN was grounded in lived experience and addressed the realities of urgent dental care.
Understanding patient experiences of urgent dental care
To understand why people avoid routine dental attendance, we carried out in-depth qualitative research in different urgent dental care settings across Merseyside.
This work included approximately 160 hours of observation of urgent dental visits, alongside interviews with 97 people experiencing dental problems. Some participants were interviewed once, while others took part in interviews over time.
During this research, we listened to people’s stories about their experiences of dental care, explored what made it difficult for them to attend the dentist routinely, and asked what might help them feel more comfortable returning for routine care or check-ups after an urgent visit. The findings from this work directly informed the development of the RETURN intervention and its supporting resources.
Barriers to routine dental visiting
Analysis of the qualitative data identified six barriers to routine dental visiting:
- Cost
- Time
- “I don’t think to go when I’m not in pain”
- Trust
- Embarrassment
- Anxiety
These barriers were not experienced in isolation and were often shaped by previous dental experiences, competing life pressures, and perceptions of dental services.
Developing the RETURN intervention
Insights from the wider literature combined with qualitative research were used to design a brief behavioural intervention that could be delivered by a dental nurse during an urgent dental care appointment.
The intervention was designed to support a non-judgemental, empathic discussion between the dental nurse and the patient, focusing on the patient’s own barriers to dental visiting. There is no fixed script for this conversation; instead, the emphasis is on asking open questions, listening, and supporting patients to reflect on their concerns.
The intervention comprised the following components:
- a non-judgemental, empathic discussion with a dental nurse about barriers to dental visiting
- a series of six short videos, each addressing one of the identified barriers to dental attendance
- a series of six barrier-specific booklets containing patient stories, motivational messages, and practical hints and tips for overcoming barriers
- a Next Appointment Toolkit booklet providing practical advice on making and keeping a dental appointment
- a written goal-setting and action-planning exercise facilitated by a dental nurse
These resources were designed to be used flexibly, allowing the conversation to focus on the barrier that mattered most to the patient while maintaining a consistent intervention approach.
Patient and public involvement and engagement
Alongside the qualitative research, patient and public involvement and engagement were central to Phase 1 of the RETURN programme.
Throughout the development phase, we worked with members of the public and patients to ensure that people’s voices were properly represented. This included discussions with individuals from a wide range of community groups, from young people involved in employability and welfare programmes to military veterans attending local support groups. In total, we spoke with over 300 people during this phase of the programme.
In addition to this wider engagement, a group of four patient and public representatives guided the work throughout the programme. We also worked closely with a Community Advisory Group made up of nine local people over a two-year period.

This group co-designed the intervention resources, contributed their own photographs to illustrate their experiences of dental visiting, and curated a photographic exhibition at the University of Liverpool in February 2020.
This collaborative approach helped ensure that RETURN was grounded in lived experience and responsive to the needs of people who face barriers to routine dental care.
Recognition for public involvement and engagement
The RETURN programme received recognition for its work with patients and local communities, including:
- Health and Life Sciences Public Engagement Award, 2024 – Commended
- University of Liverpool Staff Awards for Outstanding Contribution to Public Engagement, 2022 – Finalist
- Northwest Coast Research and Innovation Awards for Outstanding Contribution to Patient and Public Involvement, 2021 – Finalist
- Tate Exchange Liverpool, 2020 – Knowledge Exchange proposal selected
- Health and Life Sciences Public Engagement Award, 2019 – Winner
Refining language, tone, and content
Before finalising the intervention resources, we worked closely with members of the public to refine the language, tone, and content. This iterative process ensured that the materials were relevant, acceptable, and genuinely useful, and that they avoided judgemental or clinical language that could deter engagement.
Feedback from patients and community members informed revisions to wording, imagery, and presentation across all materials.
Outputs from Phase 1
Two peer-reviewed publications describe this phase of the work in detail:
- Publication describing the development of the RETURN intervention
- Publication describing patient and public involvement and engagement in the RETURN programme (embed)
Phase 2: Feasibility study
Phase 3: Randomised Controlled Trial
Phase 3 involved a pragmatic randomised controlled trial to evaluate whether delivery of the RETURN intervention during urgent dental care appointments supported patients to re-engage with routine dental care (Primary outcome 1) and influenced oral health–related quality of life (Primary outcome 2), compared with usual urgent dental care alone..
The trial was embedded within real-world urgent dental care settings to assess the effectiveness of RETURN when delivered by dental nurses as part of usual urgent dental care pathways.
Trial design and setting
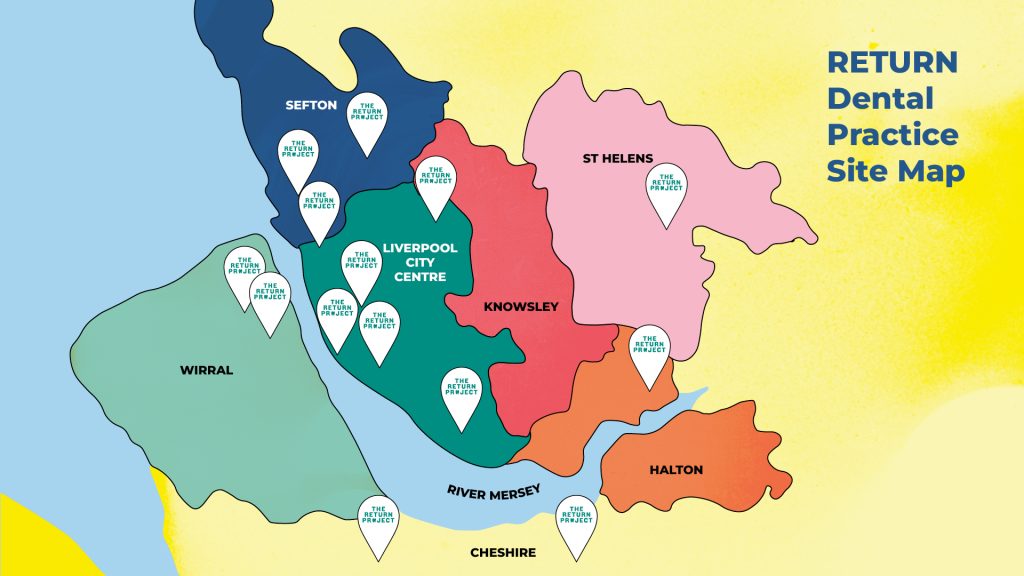
The RETURN trial commenced in August 2021, when the first participant was recruited. Recruitment took place over a 13-month period, during which 1,180 patients were enrolled from 14 urgent dental care sites.
Participating sites included:
- Liverpool Dental Hospital
- 13 dental practices providing urgent dental care during usual working hours
- 1 urgent dental clinic providing care outside of usual working hours
These sites were selected to reflect variation in urgent dental care provision.
Intervention delivery and training
A total of 14 dental nurses were trained to deliver the RETURN intervention as part of the trial. Training focused on supporting dental nurses to use the intervention resources as intended, engage patients in a non-judgemental and empathic conversation, and integrate delivery within urgent care workflows.
The intervention was delivered during urgent dental care appointments and was designed to take approximately 15 minutes.
- an intervention group, who received the RETURN intervention alongside their urgent dental care appointment
- a control group, who received usual urgent dental care only
- participant-reported questionnaire measures
- routinely collected NHS dental data
- return to routine dental care
- oral health-related quality of life
- dental anxiety
- prescriptions for painkillers or antibiotics for dental problems
- use of non-dental services for dental problems (e.g. GP or A&E attendance)
Response rates for participant-reported outcomes were:
- 6 months: 72%
- 12 months: 67%
- 18 months: 59%